Socials







September 24, 2025
Earwax: The Overlooked Health Indicator
Most people treat earwax as something to remove. In fact it is a protective coating that traps dust and microbes, keeps the ear canal skin conditioned, and supports a slightly acidic environment that discourages infection. Noticing its type, texture, color, and smell can offer practical clues about skin health, hygiene habits, and the risk of blockage. Earwax comes from ceruminous and sebaceous glands and contains lipids, proteins, salts, and natural antimicrobials that help defend the outer ear (Stone and Fulghum 1984; Schwartz et al. 2017).
Why earwax matters
Earwax is part of the first line of defense for hearing health. Laboratory studies describe bactericidal activity in human cerumen, while clinical guidance notes that overcleaning removes this barrier and raises infection risk by drying and irritating the canal skin (Stone and Fulghum 1984; Schwartz et al. 2017). The ear canal also has a self cleaning conveyor. As new skin grows outward from the ear drum, old wax normally migrates to the opening where it falls away during washing. Problems arise when wax is compacted, when devices block migration, or when skin is inflamed.
What variation can tell you
Type and texture
Wet wax is sticky and yellow to brown. It traps debris effectively but can build up faster. Dry wax is gray and flaky. It sheds more easily but the canal may feel itchy if you overclean. Both are normal. A single nucleotide change in the ABCC11 gene explains most of the wet versus dry difference across people, but daily care recommendations are similar for both types (Yoshiura et al. 2006).
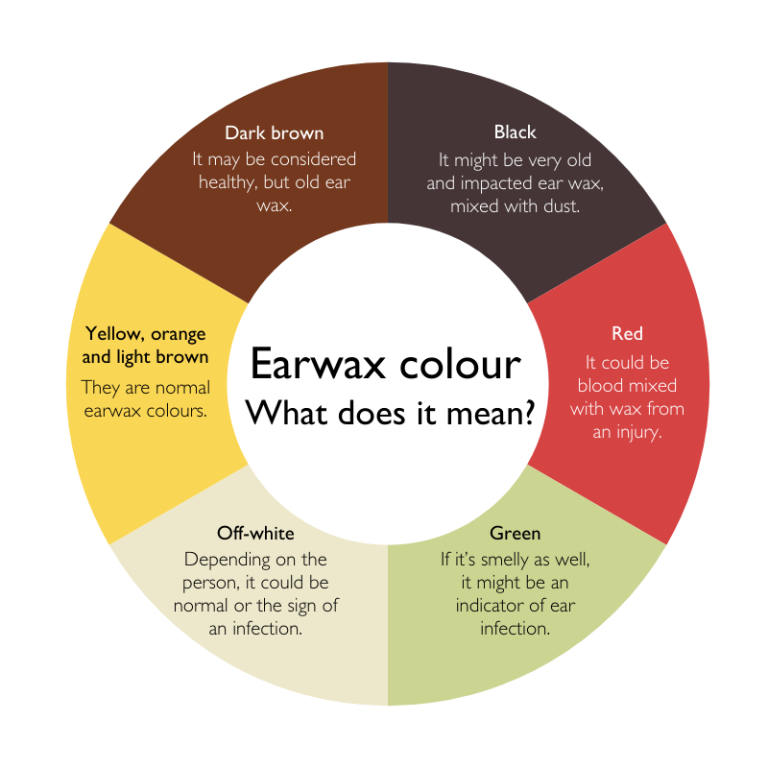
Color
Pale yellow to honey brown is usual. Very dark brown often means older oxidized wax. Green or a reddish streak can point to infection or minor bleeding and deserves attention if persistent. Chalky white flakes may suggest very dry skin or dermatitis. Color is a guide and should be read alongside symptoms such as pain, itch, or hearing change.
Smell
Fresh wax has a mild scent. Strong or foul odor with discharge or pain signals possible infection and needs assessment. Genetics that influence axillary odor also relate to earwax chemistry, yet odor alone is not diagnostic and context matters (Yoshiura et al. 2006; Schwartz et al. 2017).
Symptoms that pair with wax clues
A sense of fullness, pressure, or muffled hearing suggests compaction. Itch without pain often reflects dry skin. Sharp pain or fever points toward otitis externa rather than a wax issue. Tinnitus or brief dizziness can occur with impaction and usually improves after safe removal by a clinician.
Everyday care that protects the canal
Clean the outside only
Wipe the outer ear with a damp cloth in the shower and let water drain out. Do not insert cotton swabs. Swabs push wax deeper and can abrade the canal skin, increasing infection risk and causing impaction.
Soften before clearing
If the ear feels blocked, use a few drops of mineral oil, baby oil, glycerin, or saline nightly for several days. Softening reduces friction and often restores natural migration. People with a perforated ear drum, prior ear surgery, ear tubes, severe pain, or drainage should not self irrigate and should seek care first.
Irrigate wisely
If you have an intact ear drum and no history of ear disease, gentle body temperature water irrigation with a bulb syringe can help after softening. Tilt the head, use moderate pressure, and let water flow out freely. Stop if you feel pain or dizziness. Dry the ear afterward. Avoid powered jet devices unless under clinical supervision.
Manage device time
Earplugs, hearing aids, and in ear headphones can trap wax and moisture. Give the canal breaks when possible. Clean tips, domes, and filters regularly. Hearing aid users often benefit from scheduled professional cleaning to prevent feedback and irritation.
Care for the skin
If you swim often or sweat heavily, rinse and dry the outer ear after activity. For recurrent itch without infection, a clinician may suggest short courses of emollients or prescription drops for dermatitis. Avoid perfume heavy products that can irritate thin canal skin. Consider room humidification during very dry seasons.
Patterns and what they may indicate
Frequent thick buildup
Common with wet type wax, narrow canals, hearing aid use, or habitual swabbing. Plan routine softening and periodic professional removal. Review device fit and ventilation if you use ear inserts daily.
Flaky itchy canals
Seen with dry type wax and with eczema or psoriasis. Overcleaning worsens this pattern. Keep cleaning to the outside, consider gentle emollients if advised, and seek care for persistent redness or crusting that suggests dermatitis or fungal growth.
Bad smell with drainage and pain
Suggests otitis externa rather than a wax problem. This requires medical treatment with topical drops. Do not irrigate a painful draining ear and keep the ear dry until reviewed.
Hearing worse after showers
Water can swell wax and temporarily block sound. Many people improve with softening and careful irrigation when appropriate. If one ear is consistently worse, have it examined to rule out asymmetry or a foreign body.

Safe self care checklist
- Keep swabs out of the canal and clean only the outer ear.
- If blocked, soften with a few drops nightly for three to five nights.
- If eligible, irrigate gently with body temperature water and stop if painful.
- Dry the ear after water exposure and limit prolonged moisture.
- Clean hearing devices regularly and schedule maintenance.
- Seek care for pain, discharge, fever, sudden hearing loss, dizziness, or symptoms that last beyond one to two weeks.
When to see a clinician
Get assessed if you have severe pain, spreading redness, fever, persistent drainage, sudden hearing loss, dizziness, a known perforation, prior ear surgery, or if home measures fail. Children, people with diabetes, those on anticoagulants, and people with immune compromise should be cautious with self care and engage clinicians early. Professionals can remove wax safely with curettes, suction, or controlled irrigation and can treat underlying skin conditions that cause recurrence. This restores clear hearing, reduces itch and odor, and prevents avoidable injury from self instrumentation.
The takeaway
Earwax protects the ear canal and offers useful signals when you know what to look for. Preserve the barrier. Avoid digging. Use softening and careful irrigation only when appropriate. Ask for help when symptoms suggest infection or when you are unsure. Small habits keep the canal healthy and your hearing clear.
References
Schwartz SR, Magit AE, Rosenfeld RM et al. 2017 Clinical practice guideline. Earwax cerumen impaction update. Otolaryngology Head and Neck Surgery 156 1 Suppl S1 S29. https://doi.org/10.1177/0194599816671491
Stone M and Fulghum RS 1984 Bactericidal activity of wet cerumen. The Laryngoscope 94 364 367. https://doi.org/10.1288/00005537-198403000-00019
Yoshiura K, Kinoshita A, Ishida T et al. 2006 A SNP in the ABCC11 gene is the determinant of human earwax type. Nature Genetics 38 324 330. https://doi.org/10.1038/ng1733

Earwax protects ears and signals health. Type, color, and smell offer clues. Skip swabs, soften gently, and seek care if painful.










